

Lisa Bowernan
Janelle White
Neurological Disorders
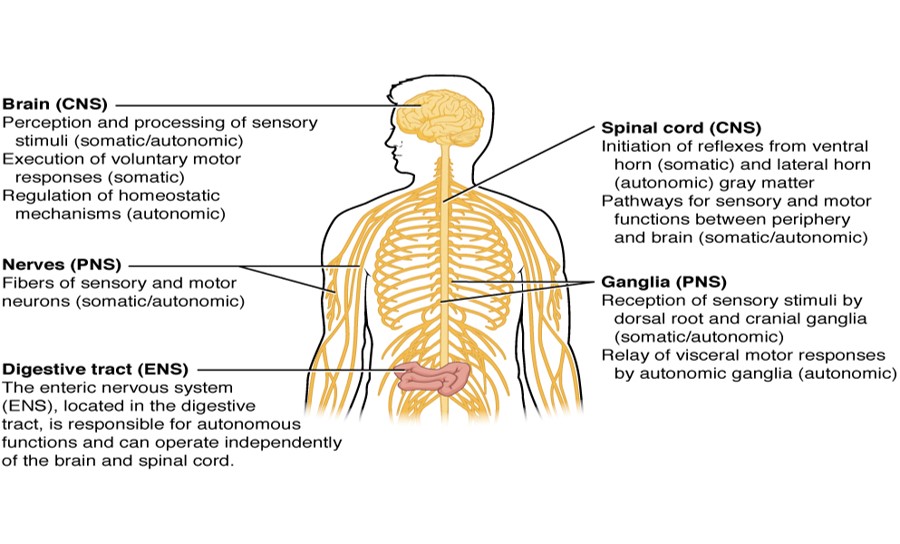
This image is licensed under the Creative Commons Attribution 3.0 Unported license: Attributed to OpenStax College via wikimedia commons
- Basic Functions of NS
- NS – 2 divisions…
- CNS…
- Brain…
- Blood supply…
- BBB…
- RAS…
- Spinal cord…
- PNS…
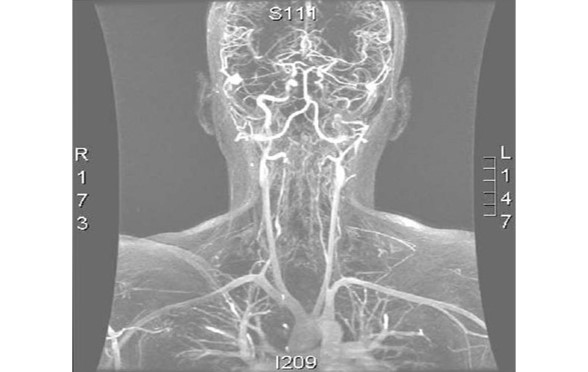
"Angio MR" by Germain Orphanet Journal of Rare Diseases 2007 2:32 doi:10.1186/1750-1172-2-32. Licensed under CC BY 2.0 via Wikimedia Commons
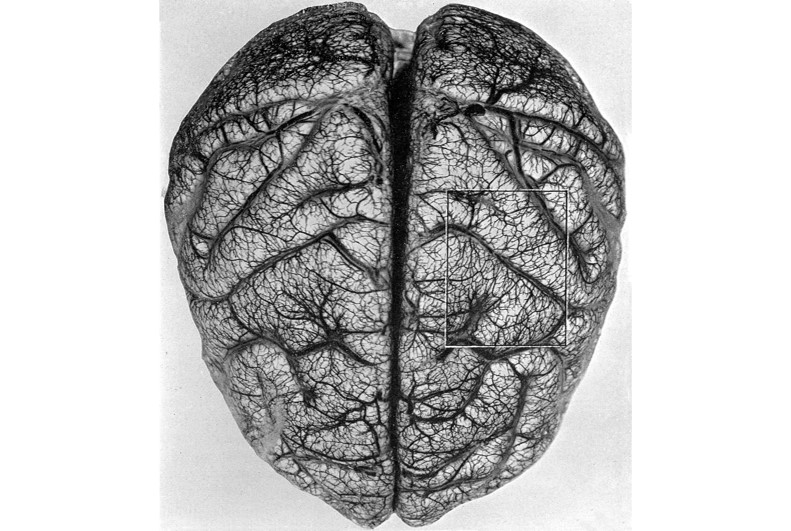
Arteries and veins of the brain. Wellcome Library, London [CC BY 4.0], via Wikimedia Commons

This work is in the Public Domain.
Attribution: Rhcastilhos (Gray519.png) [Public domain],
Sourced via Wikimedia Commons
"Confusion" is licensed under the Creative Commons Attribution-NonCommercial-NoDevivs 2.0 license: Attributed to Smythe Richbourg
- Definition?
- How do we determine if our patient has an AMS?
- What tools do we have to use?
Fully reversible brain injury that does not involve any bruising or structural damage to the brain.
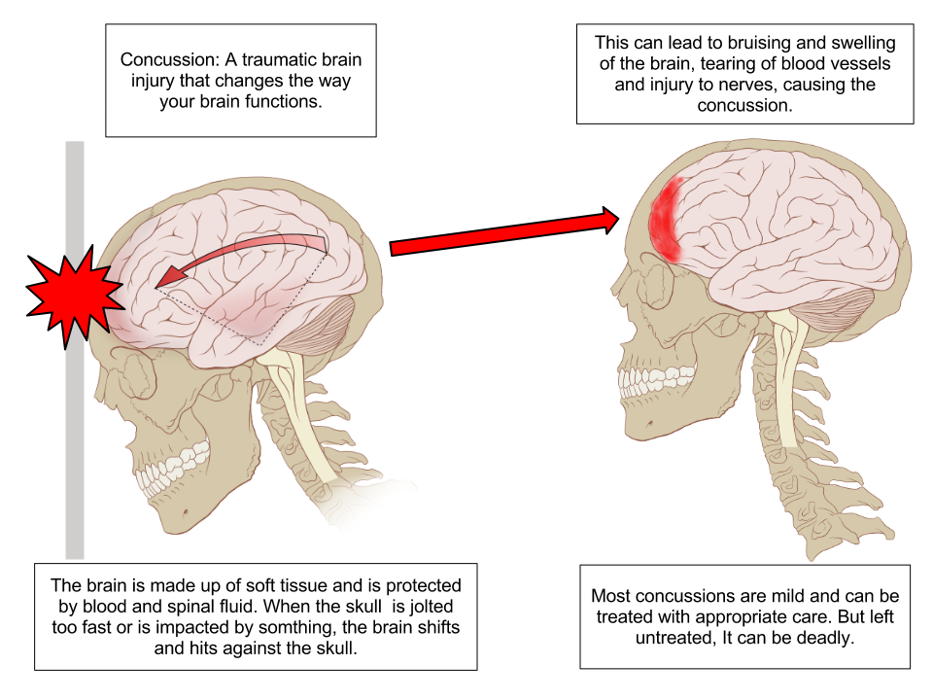
"Concussion Anatomy" is licensed under the Creative Commons Attribution-Share Alike 3.0 license: Attributed to Max Andrews via Wikimedia Commons

Utah cowboy (explored) is licensed under the Creative Commons Attribution-NonCommercial 2.0 Unported license: Attributed to Elizabeth Haslam
- Mild to moderate impact to skull
- Brief LOC (< 5 min)
- Temporary disturbance of function
- ? Mild Retrograde amnesia
- Drowsiness, irritability, confusion.
- True concussion – does not get worse!
- A lucid interval = a temporary improvement in a patient's condition after a TBI, after which the condition deteriorates, sometimes rapidly.
- A lucid interval is especially indicative of an epidural haematoma.
- An estimated 20 to 50% of patients with epidural haematoma experience a lucid interval
Retrograde Amnesia: No memory of what happened just before an event
Anterograde Amnesia (for interest only): inability to create new memories post event

Acid Queen is licensed under the Creative Commons Attribution 2.0 license: Attributed to Ian Burt
Definition…
“What’s blood got to do, got to do with it!”
4 Broad Causes:
- Blood oxygenation problems?
- Blood circulation problems?
- Metabolic problems?
- CNS problems?
May be a combination, such as?

This image adapted from 24k Jumping Brain is licensed under the Creative Commons Attribution-NonCommercial 2.0 license: Attributed to Emillio Garcia
- The brain represents only 2% of body weight
- It receives 15% of the cardiac output
- Uses 20% of total body oxygen consumption and
- Uses 25% of total body glucose.

Myasthenia is licensed under the Creative Commons Attribution- Share Alike 3.0Unported license: Attributed to Cumulus
Managing the business
F.A.S.T
Decreased LOC
Unequal pupils
Facial droop
Inability to speak
Paralysis (hemiplegia)
Loss of bladder control (incontinence)
Other S&S not necessarily presented in this case…….
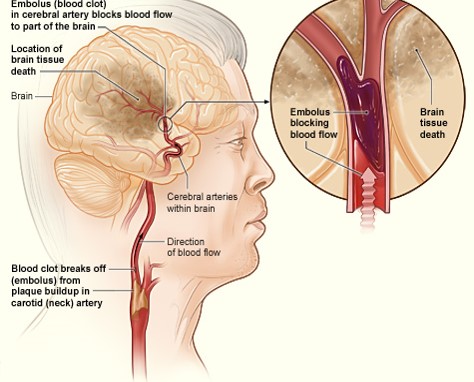
Ischemic Stroke By National Heart Lung and Blood Institute (NIH) (National Heart Lung and Blood Institute (NIH)) [Public domain], via Wikimedia Commons.
Cerebral artery is blocked by a clot or other foreign matter
- Thrombotic stroke (most common type)
- The narrowing and eventual occultion often occurs over a long period of time - S&S much slower,
- Headache not commn
- Embolic stroke
- Usually originates from the carotid artery or the heart (AF) - clot travels unit it lodges in a small cerebral artery blocking blood flow.
- Onset of S&S more sudden - headache, seizure activity or brief periods of unresponsiveness are more common
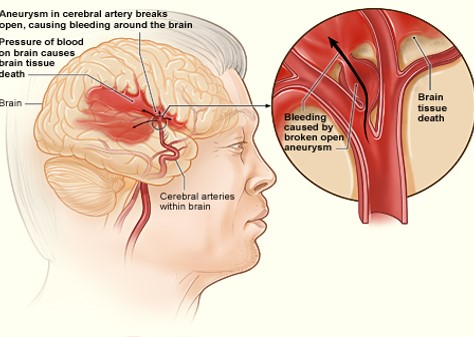
Haemorrhagic Stroke By National Heart Lung and Blood Institute (NIH) (National Heart Lung and Blood Institute (NIH)) [Public domain], via Wikimedia Commons.
- Rupture of an artery causing bleeding within the brain ICH or in the space around the outer surface of the brain SAH
- Often associated with hypertension
- Subarachnoid (SAH) often associated with aneurysms
- SAH commonly due to trauma
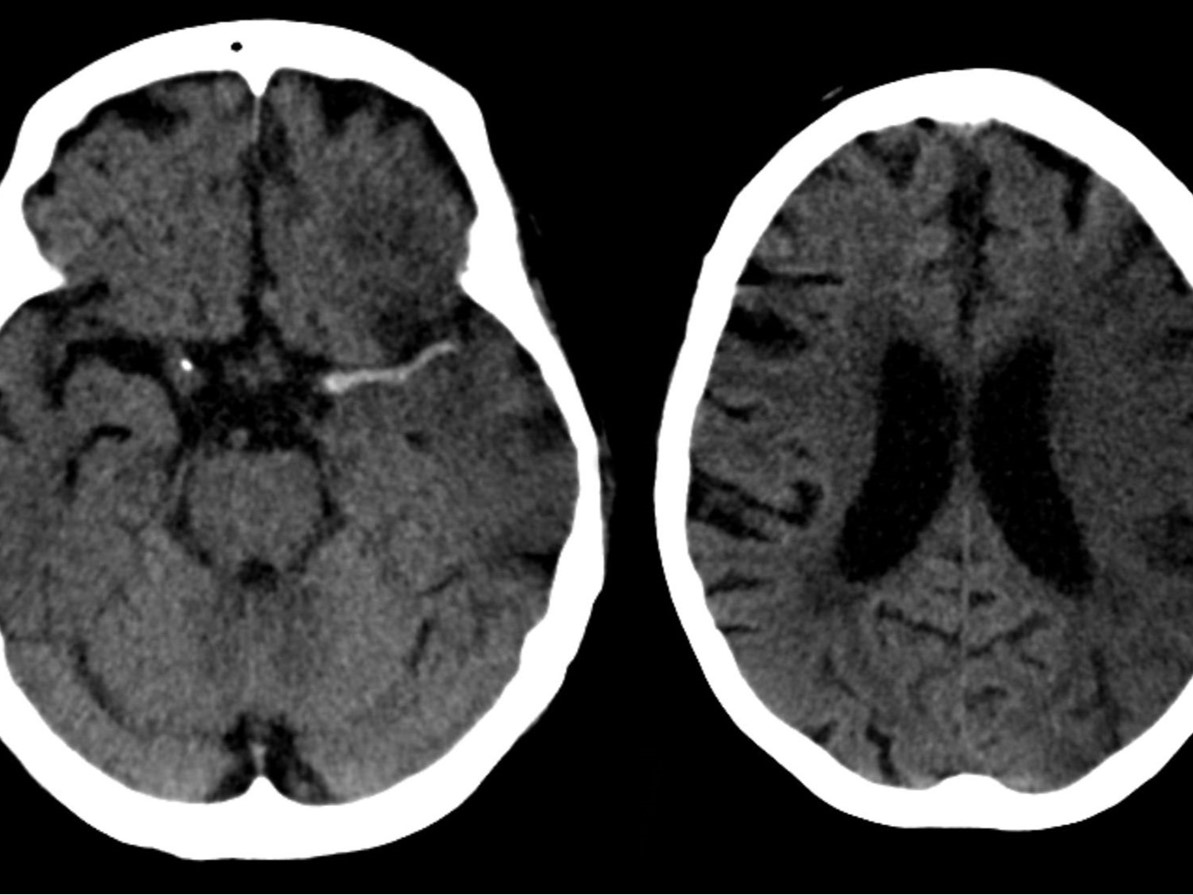
Left image: Haemorrhage.
Right image: Ischaemia.
This image is licensed under the Creative Commons Attribution- Share Alike 3.0 Unported license: Attributed to Hellerhoff via Wikimedia commons
This image is licensed under the Creative Commons Attribution -Share Alike 3.0 Unported license: Attributed to Kevjonesin via wikimedia commons
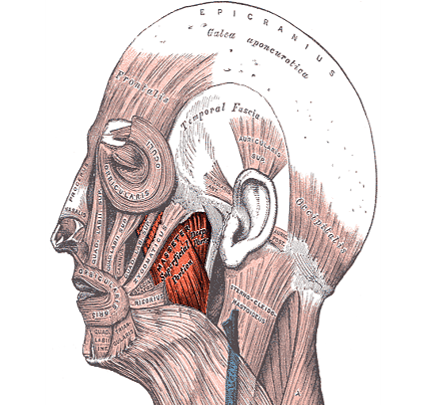
(Tension Type Headache)
The most common!

This image is in the public domain
-
Brain tumour
-
SAH
-
ICH
-
Meningitis
-
Hypertension
-
Hypoglycaemia
-
CO poisoning, other toxic inhalation
-
Fever
-
Hypoxaemia
-
Stroke
-
Depression

![Creative Commons Licence [Some Rights Reserved]](http://creativecommons.org/images/public/somerights20.gif) © Copyright Peter Jeffery and
licensed for reuse under this Creative Commons Licence.
© Copyright Peter Jeffery and
licensed for reuse under this Creative Commons Licence.
- You are called to the local cricket ground to a 29 year old male pt having a ?seizure
- You find your pt lying on his side?
- As approach you note there are no dangers

Adapted from Think by Sam Howzit licensed under a Creative Commons Attribution 3.0 Unported License.
-
Pt unresponsive to verbal stimuli
-
Pt withdraws from painful stimuli
-
RR – 14 & deep, note loud snoring
-
Pulse - 112
-
Skin pink, warm, moist
Bystanders provide the following information
“One minute he was playing cricket when all of a sudden he collapsed to the ground and began shaking all over”.

This image is licensed under the Creative Commons Attribution-ShareAlike 2.0 Unported license: Attributed to William Murphy
It's a hot summers day at 1500hrs, when you are called to a person collapsed at the local RSL.
- What provisional diagnosis is going through your mind?
- What do you do when you arrive on scene?

This image is in the public domain
- Nil Danger noted
- Responds to verbal command- however seems a little vague
- Responds appropriately when you ask who and where she is.
- RR – 22 regular, nil dyspnoea
- Weak radial pulse 102, regular
- Skin cool, moist, pale.
- TESTS?
- THOUGHTS?
- QUESTIONS?
Associated with LQTS & V-Arrythmias: (Antiarrhythmic, gastric motility promoters, Antibiotics) quinidine, sotalol, amiodarone, procainamide, erythromycin, haloperidol, tricyclic antidepressants.
Associated with Bradycardia: (Beta-blockers, Na channel blockers) verapamil, dilatiazem, digoxin.
Associated with Postural Hypotension: (Anti-hypertensive drugs, anti-Parkinson and diuretics) prazosin, Ca channel blockers, furosemide, nitrates.

This image is in the public domain
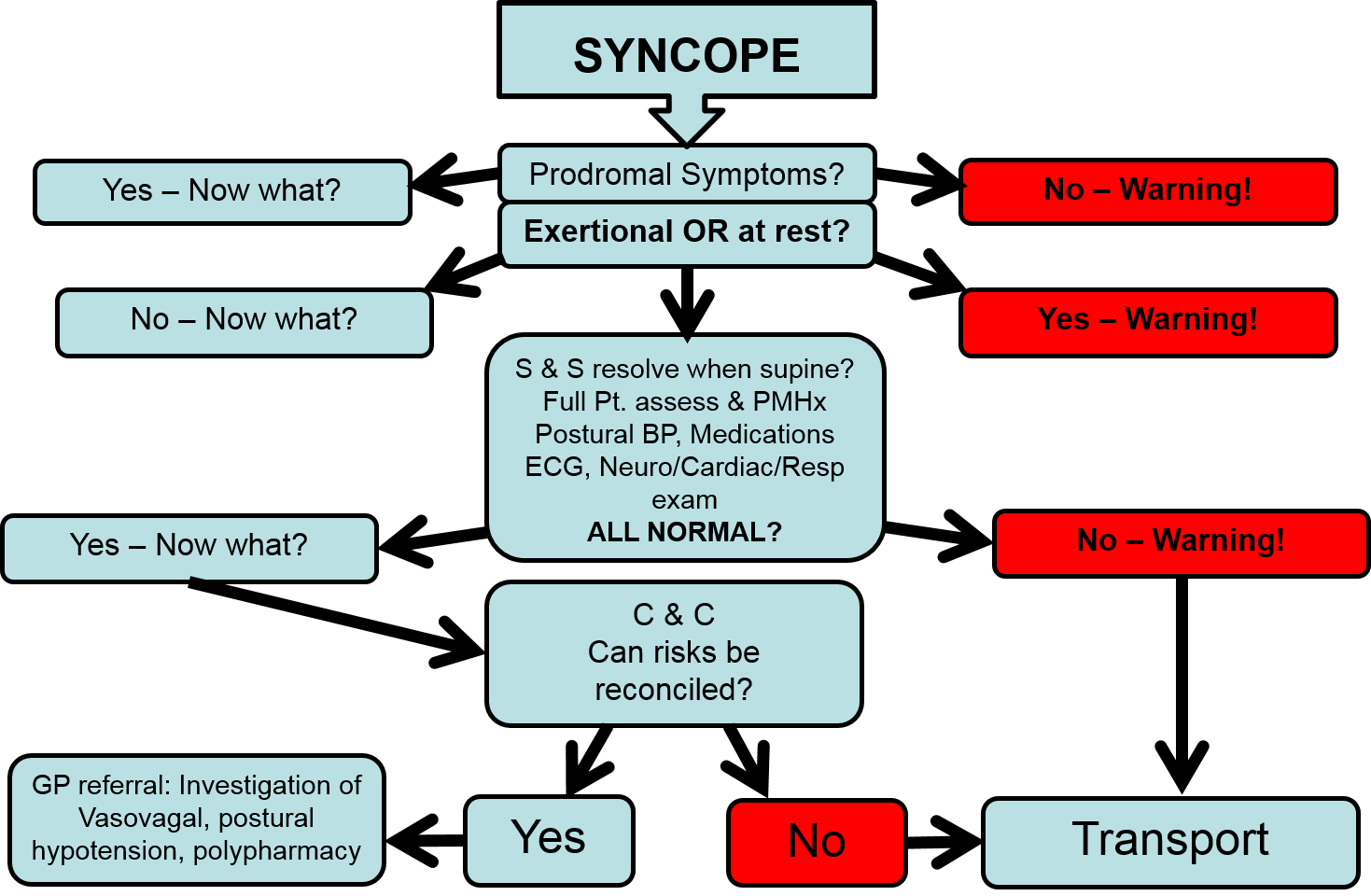
7 common Prodromal S & S
- Diaphoresis
- Pallor
- Nausea
- Palpitations
- Visual disturbance
- Hearing disturbance
- Dizziness
This image is licensed under the Creative Commons Attribution 2.0 license: Attributed to SOCIALisBETTER
- Review Neurological A & P
- Pathophysiology
- AMS
- Unconsciousness
- Common neurological conditions
- CVA/TIA
- Headache
- Seizures
- Syncope
The next slide will have removed your chosen card
Click here to see the next slide

Except where otherwise noted, content on this page is licensed under a Creative Commons Attribution-ShareAlike 4.0 International Licence
Note: The open version of this document may have been altered from the original. Only pages on this site that display the CC licence and logo are licensed under a Creative Commons licence.
| Attribution information | |
|---|---|
| Title: | Lecture Slides: 'CAA108' - Open Version |
| Source: | https://www.utas.edu.au/health/resources/open-resources/resources/courses/paramedicine/caa108-lecture-slides |
| Author: | Dr Lisa Bowerman |